
Pes Anserinus Pain in Runners: Understanding Causes, Diagnosis & Recovery
- endurancehealthlab
- Jun 11, 2025
- 5 min read

Updated: Jun 24, 2025
Inner knee pain, especially just below the joint line, is a common complaint among runners. While medial meniscus or MCL injuries are often suspected, pes anserinus tendinopathy or bursitis is a frequently overlooked, but treatable condition affecting the tendons and bursa on the anteromedial tibia.

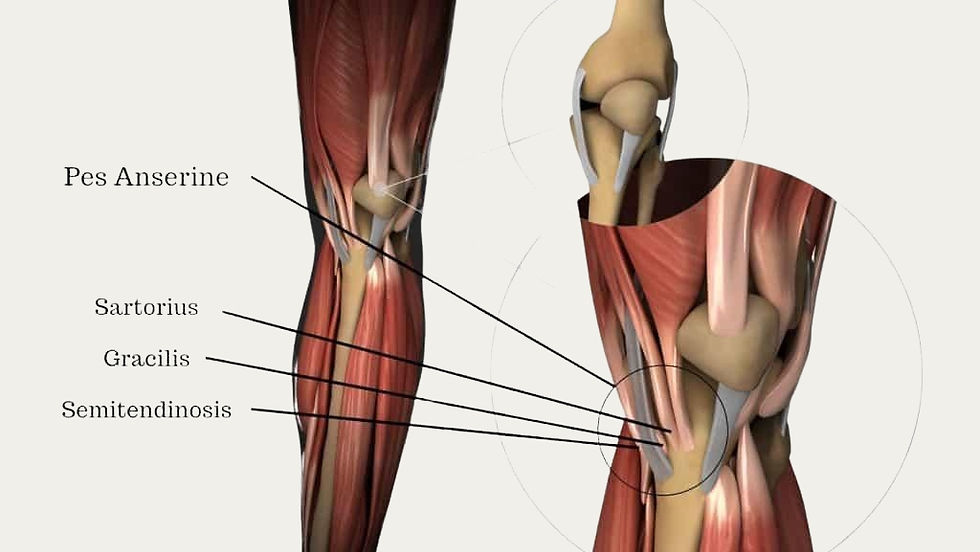
What Is the Pes Anserinus?
The pes anserinus ("goose's foot") refers to the insertion of three muscles:
Sartorius
Gracilis
Semitendinosus
Why Runners Are Susceptible: The Biomechanics
1. Repetitive Stress and Flexion Cycles
Runners perform up to 1,500 strides per kilometre, subjecting the hamstrings and adductors to repetitive eccentric and concentric loads (Alvarez-Nemegyei, 2007; Homayouni et al., 2016).
2. Dynamic Valgus and Gluteal Weakness
Poor gluteus medius activation leads to hip adduction and internal rotation, causing the knee to collapse inward (valgus). This increases friction and tensile strain on the pes tendons (Aicale et al., 2024; Sarifakioglu et al., 2016).
3. Foot Mechanics
Excessive pronation causes tibial internal rotation, stressing the insertion point and increasing bursal compression (Alvarez-Nemegyei, 2007; Yoon et al., 2005).
4. Load Errors
A systematic review by Choi et al. (2021) identified training volume spikes and poor recovery as major contributors to overload-related tendon injuries in runners.
Symptoms and Clinical Presentation
Pain 4–5 cm below the medial joint line
Worse with stairs, kneeling, or getting out of a car
Pain on resisted knee flexion, hip adduction or passive extension with valgus stress
Occasional swelling or burning over the insertion (Rennie & Saifuddin, 2005)
Differential Diagnosis
Differentiating Pes Anserinus disorders from other medial knee pathologies is crucial:
Condition | Key Features |
Pes Anserinus Bursitis | Pain localised below the joint line; tenderness over the pes anserinus area. |
Medial Meniscus Tear | Joint line tenderness; possible locking or clicking sensations. |
MCL Sprain | Pain over the medial collateral ligament; instability during lateral movements. |

Diagnosis and Imaging
Clinical Testing
Palpation: Focal tenderness at the pes insertion
Pain reproduction: Resisted knee flexion or internal rotation, passive stretch, or valgus load
Differential tests: McMurray's or valgus stress test to rule out meniscal or MCL involvement (Medscape, 2024)
Ultrasound
Reveals bursal distension, tendon thickening, and increased Doppler flow - useful for confirming diagnosis and guiding injections (Yoon et al., 2005).
MRI
Used in chronic or complex cases to rule out intra-articular involvement. Findings include soft tissue edema and peritendinous inflammation (Radiopaedia, 2024).
Diagnostic Injection
An anesthetic injection into the bursa that resolves symptoms confirms pes anserinus bursitis as the pain source (Medscape, 2024).
3-Phase Rehabilitation Plan: Pes Anserinus Pain
Phase I - Settle Symptoms (1–2 weeks)
Goals: Reduce pain and inflammation, protect from further aggravation
Interventions:
Relative rest and activity modification (avoid stairs, deep squats)
Ice and NSAIDs if needed
Manual therapy to release hamstrings, adductors
Isometric exercises
Education on load management
Kinesiotaping plus isometrics reduced symptoms comparably to NSAIDs (Homayouni et al., 2016).
Phase II - Restore Strength and Mobility (2–4 weeks)
Goals: Restore normal movement patterns and build load tolerance
Interventions:
Glute medius and glute max strengthening
Hamstring and adductor eccentrics
Hip mobility
Gait retraining if valgus collapse or overstriding is present
Introduce unilateral strengthening and proprioception
Physiotherapy was superior to corticosteroid injections over 6 weeks (Sarifakioglu et al., 2016).
Prolotherapy and corticosteroids showed varying timelines of effectiveness (Babaei-Ghazani et al., 2024).
Phase III - Return to Running (4–6+ weeks)
Goals: Safely reintroduce running and high loads
Interventions:
Walk-run progression
Introduce plyometrics
Continue strength training (2x/week maintenance)
Shoe and orthotic review for pronation control
Daily movement pattern modification helped reduce symptoms (Farsad et al., 2023).
Key Takeaways
Common in runners due to repetitive valgus stress, poor hip control, and overuse.
Presents with localised medial knee pain below the joint line, worsened by stairs, running, or resisted knee flexion.
Clinical exam is primary; ultrasound and MRI assist in complex or persistent cases.
Often linked to weak glutes, poor hip stability, excessive foot pronation, and altered running mechanics.
Treatment involves load management, hip/core strengthening, gait retraining, and gradual return to sport.
Prognosis is excellent with comprehensive rehab addressing the kinetic chain.
Biomechanical corrections (hip, foot, gait) are key to preventing recurrence.

When to See a Physiotherapist at Endurance Health Lab
You should consider seeing a physiotherapist if you experience:
Localised pain on the inside of the knee or upper shin that worsens with running
Pain during walking, stairs, or hopping
Persistent symptoms despite rest, footwear changes, or self-management
A recent increase in running distance, speed, or hill training
Difficulty returning to sport due to recurring knee discomfort
📅 Book an assessment with Endurance Health Lab. We’ll guide you through accurate diagnosis, imaging referral if needed, and a personalised return-to-running program that ensures long-term recovery.
Located in Chatswood, 2067
📚 References
Aicale, R., Pellegrino, R., Di Iorio, A., Mottola, R., Saggini, R., Ruosi, C., & Tarantino, D. (2024). Comprehensive review of pes anserinus syndrome: Etiology, diagnosis, and management. European Journal of Musculoskeletal Diseases, 13(3), 60–69.
Alvarez-Nemegyei J. (2007). Risk factors for pes anserinus tendinitis/bursitis syndrome: a case control study. Journal of clinical rheumatology : practical reports on rheumatic & musculoskeletal diseases, 13(2), 63–65.
Babaei-Ghazani, A., Eftekharsadat, B., Soleymanzadeh, H., & ZoghAli, M. (2024). Ultrasound-Guided Pes Anserine Bursitis Injection Choices: Prolotherapy or Oxygen-Ozone or Corticosteroid: A Randomized Multicenter Clinical Trial. American journal of physical medicine & rehabilitation, 103(4), 310–317.
Choi, H. J., Back, H. K., Kim, Y. J., Oh, D. Y., Park, C. W., & Namgoong, J. (2021). A review of randomized controlled trials of pes anserinus tendinitis/bursitis syndrome in the China National Knowledge Infrastructure database. Journal of Acupuncture Research, 38(4), 284–292.
Farsad, F., Moghimi, J., Mirmohammadkhani, M., Gholami, E., & Moazeni, M. (2023). The effect of modifying the sitting and getting up method on pain intensity in patients with pes anserine tendinitis bursitis: A randomized clinical trial study [Preprint]. Research Square.
Homayouni, K., Foruzi, S., & Kalhori, F. (2016). Effects of kinesiotaping versus non-steroidal anti-inflammatory drugs and physical therapy for treatment of pes anserinus tendino-bursitis: A randomized comparative clinical trial. The Physician and sportsmedicine, 44(3), 252–256.
Khosrawi, S., Taheri, P., & Ketabi, M. (2017). Investigating the Effect of Extracorporeal Shock Wave Therapy on Reducing Chronic Pain in Patients with Pes Anserine Bursitis: A Randomized, Clinical- Controlled Trial. Advanced Biomedical Research, 6, 70.
Medscape. (2024). Pes anserine bursitis – Clinical presentation. Medscape Reference. https://emedicine.medscape.com/article/308694-clinical
Radiopaedia. (2024). Pes anserine bursitis. Radiopaedia.org. https://radiopaedia.org/articles/pes-anserinus-bursitis-1
Rennie, W. J., & Saifuddin, A. (2005). Pes anserine bursitis: incidence in symptomatic knees and clinical presentation. Skeletal radiology, 34(7), 395–398.
Sarifakioglu, B., Afsar, S. I., Yalbuzdag, S. A., Ustaömer, K., & Bayramoğlu, M. (2016). Comparison of the efficacy of physical therapy and corticosteroid injection in the treatment of pes anserine tendino-bursitis. Journal of physical therapy science, 28(7), 1993–1997.
Yoon, H. S., Kim, S. E., Suh, Y. R., Seo, Y. I., & Kim, H. A. (2005). Correlation between ultrasonographic findings and the response to corticosteroid injection in pes anserinus tendinobursitis syndrome in knee osteoarthritis patients. Journal of Korean medical science, 20(1), 109–112.



The article presents a thorough examination of pes anserinus disorders, highlighting the often overlooked causes of inner knee pain in runners. Notably, the mention of training volume spikes is critical in understanding injury prevention strategies. The discussion around Pay ID as a method of financial transaction could also be mirrored in healthcare, where integrating payment systems might streamline access to physiotherapy services. Understanding these connections is vital for holistic management.